Trainings and Presentations
Project staff facilitate trainings and presentations around the topic of suicide. Common presentation topics include Resources for Youth Suicide Prevention, 988 in Indian Country, Caring Text Messages Suicide Prevention Intervention, and Media and Marketing for Veteran’s Suicide Prevention. The THRIVE team are trainers for two of the most widespread suicide intervention gatekeeper trainings: QPR (Question Persuade Refer) and ASIST (Applied Suicide Intervention Skills Training). These trainings are offered at low- or no-cost for NPAIHB member tribes. To request a training or presentation, please contact project director Colbie Caughlan at ccaughlan@npaihb.org.
Preventing Injury through Social Marketing
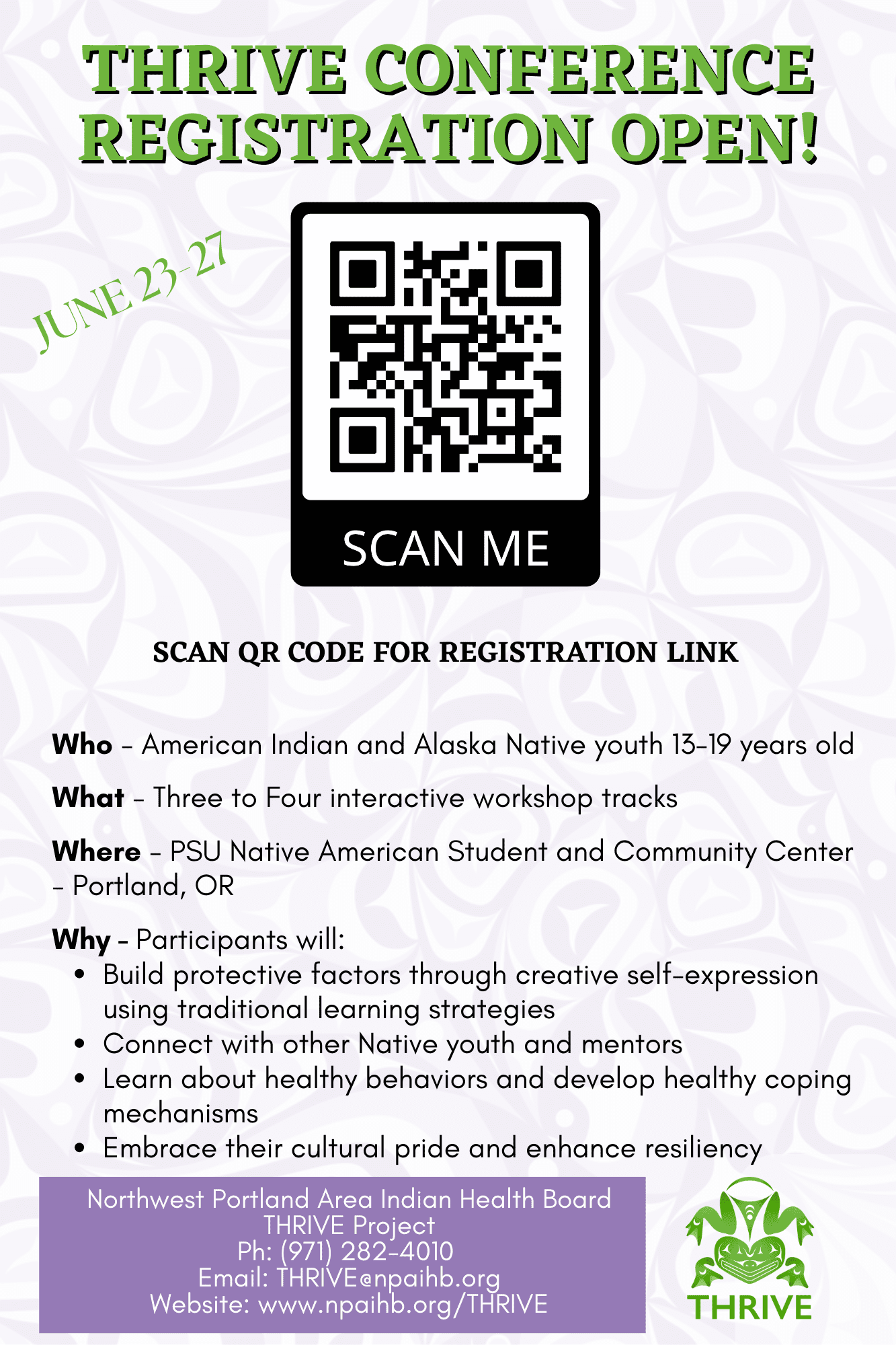
Annual THRIVE Conference
This annual summer conference is for Native youth ages 13-19 from all over Indian Country. The conference brings youth together to learn about health promotion and disease prevention with a strong focus on suicide prevention and mental health. To learn more about the THRIVE Conference please view the “THRIVE Conference” tab.
Caring Text Message Intervention Campaigns
Caring Text Messages is an evidence-based behavioral intervention and social marketing campaign, developed by the THRIVE team with the help of Native teens, college students, and Veterans. Native youth from anywhere can text “CARING’’ to 65664 to receive two texts per week with hopeful and encouraging videos, songs, and messages. Caring Messages that “express unconditional care and concern have been shown to prevent suicide deaths, attempts, ideation, and hospitalizations”. Fliers and postcards to promote the campaign are also downloadable from Healthy Native Youth’s website, www.healthynativeyouth.org (currently under construction). For the college caring text messages text “COLLEGE” to 65664 and for the Veterans text messages text “VETERAN” to 65664.
Mind 4 Health
Mind4Health is a text message service for caring adults that builds their capacity to facilitate conversations with youth to nurture mental health. The gatekeeper training was designed by the THRIVE team, to meet a need from adults who work with AI/AN youth, to help community gatekeepers identify youth in need of support and connect them to appropriate services. The series walks participants through three steps to fill their mental health toolbox. The Mind4Health training’s videos and handouts are available on Healthy Native Youth’s website, www.healthnativeyouth.org (currently under construction). Collectively, the evaluations of these programs (i.e., Caring Text Messages, BRAVE, and Mind 4 Health) indicate that behavioral interventions can be feasibly delivered via text message to AI/AN communities and that including Native youth in the formative research is critical to designing comprehensive, culturally-responsive interventions. Access Mind4Health here. (Site under construction)
The Zero Suicide Model (ZS)
The THRIVE team hosted a webinar to introduce the Zero Suicide model to new staff at the clinics we are assisting with Zero Suicide implementation. Feel free to check this webinar out and learn about the model!
.
Creative Design with Special guest – Native artist Jared Yazzie, OXDX
Youth created four meaningful social marketing campaigns by creating their own logos using digital designs inspired by the environment, culture, body and mind. Native youth amplified the advocacy for Missing and Murdered Indigenous Women, honoring tribal elders and sharing teaching passed down to them, reclaiming tribal identity through their ancestors, and being mindful of the environment and mother earth.
- MMIWG (Murdered Missing Indigenous Women and Girls)
- Life is Sacred
- Defined by my Ancestors, Not Dead Presidents
- Elder Teachings



The Beats, Lyrics, Leaders (BLL)
The Beats, Lyrics, Leaders (BLL) music track lead by recording artist J Ross Parrelli and a team of talented mentors guided youth to share their powerful voices and stories. Each participant created their own musical lyrics, created their own beats and rhythms, engaged in public speaking, and collaborate in developing an electrifying music video called “So Native.” This unified video is very powerful in sharing their cultural pride and resiliency.


Storytelling in Graphic Novels (culture as prevention)
Youth developed a graphic novel using indigenous storytelling, the Trickster story to discuss and learn the impact of substance abuse disorder and addiction in Native communities. Each story represented oral teachings from their respective communities passed from generation to generation.


Traditional Foods (culture & nutrition)
Youth prepared a healthy snack using traditional foods, hike through an urban forest making connection with indigenous plants, and participate in a service learning project to remove invasive species and protect biodiversity and water quality.

Science and Medical Track (Oregon Health and Science University)
The science and health track with Oregon Health and Science University (OHSU) exposed youth to different health and science fields at OHSU campus. The workshop provides a connection for youth who are interested in health professions and becoming future healers. Youth expressed interest in the respective fields, pharmacy, dentistry, medicine, ophthalmology, pediatrics, nursing, research, chemist, therapist, nutritionist, psychiatry, and public health!


















Trainings and Presentations
Project staff facilitate trainings and presentations around the topic of suicide. Common presentation topics include Resources for Youth Suicide Prevention, 988 in Indian Country, Caring Text Messages Suicide Prevention Intervention, and Media and Marketing for Veteran’s Suicide Prevention. The THRIVE team are trainers for two of the most widespread suicide intervention gatekeeper trainings: QPR (Question Persuade Refer) and ASIST (Applied Suicide Intervention Skills Training). These trainings are offered at low- or no-cost for NPAIHB member tribes. To request a training or presentation, please contact project director Colbie Caughlan at ccaughlan@npaihb.org.
Preventing Injury through Social Marketing
Several learning and health communication theories support the use of culturally-tailored media to increase behavior change. Tailored information is more likely to be read, understood, perceived as personally relevant, and remembered. Cultural tailoring is particularly important when addressing sensitive health topics like suicide and sexual health. To view the social marketing campaigns, please go to the Social Marketing Campaigns webpage.
Annual THRIVE Conference
This annual summer conference is for Native youth ages 13-19 from all over Indian Country. The conference brings youth together to learn about health promotion and disease prevention with a strong focus on suicide prevention and mental health. To learn more about the 2023 THRIVE Conference please scroll down and view the “THRIVE Conference” tab.
Caring Text Message Intervention Campaigns
Caring Text Messages is an evidence-based behavioral intervention and social marketing campaign, developed by the THRIVE team with the help of Native teens, college students, and Veterans. Native youth from anywhere can text “CARING’’ to 65664 to receive two texts per week with hopeful and encouraging videos, songs, and messages. Caring Messages that “express unconditional care and concern have been shown to prevent suicide deaths, attempts, ideation, and hospitalizations”. Fliers and postcards to promote the campaign are also downloadable from Healthy Native Youth’s website, www.healthynativeyouth.org. For the college caring text messages text “COLLEGE” to 65664 and for the Veterans text messages text “VETERAN” to 65664.
Mind 4 Health
Mind4Health is a text message service for caring adults that builds their capacity to facilitate conversations with youth to nurture mental health. The gatekeeper training was designed by the THRIVE team, to meet a need from adults who work with AI/AN youth, to help community gatekeepers identify youth in need of support and connect them to appropriate services. The series walks participants through three steps to fill their mental health toolbox. The Mind4Health training’s videos and handouts are available on Healthy Native Youth’s website, www.healthnativeyouth.org. Collectively, the evaluations of these programs (i.e., Caring Text Messages, BRAVE, and Mind 4 Health) indicate that behavioral interventions can be feasibly delivered via text message to AI/AN communities and that including Native youth in the formative research is critical to designing comprehensive, culturally-responsive interventions.
The Zero Suicide Model (ZS)
“The Zero Suicide Model relies on a system-wide approach to improve outcomes and close gaps. Success is achieved when clinical teams embrace the understanding that suicide deaths are preventable in their organization; and when patients feel comfortable disclosing suicide risk and work with clinic staff to lower that risk. The Model is based on the realization that suicidal individuals often fall through multiple cracks in a fragmented and sometimes distracted health care system, and on the premise that a systematic approach to quality improvement is necessary” (sprc.org). THRIVE currently has three tribal clinics implementing the ZS model.
Creative Design with Special guest – Native artist Jared Yazzie, OXDX
Youth created four meaningful social marketing campaigns by creating their own logos using digital designs inspired by the environment, culture, body and mind. Native youth amplified the advocacy for Missing and Murdered Indigenous Women, honoring tribal elders and sharing teaching passed down to them, reclaiming tribal identity through their ancestors, and being mindful of the environment and mother earth.
- MMIWG (Murdered Missing Indigenous Women and Girls)
- Life is Sacred
- Defined by my Ancestors, Not Dead Presidents
- Elder Teachings
The Beats, Lyrics, Leaders (BLL)
The Beats, Lyrics, Leaders (BLL) music track lead by recording artist J Ross Parrelli and a team of talented mentors guided youth to share their powerful voices and stories. Each participant created their own musical lyrics, created their own beats and rhythms, engaged in public speaking, and collaborate in developing an electrifying music video called “So Native.” This unified video is very powerful in sharing their cultural pride and resiliency.
Storytelling in Graphic Novels (culture as prevention)
Youth developed a graphic novel using indigenous storytelling, the Trickster story to discuss and learn the impact of substance abuse disorder and addiction in Native communities. Each story represented oral teachings from their respective communities passed from generation to generation.
Traditional Foods (culture & nutrition)
Youth prepared a healthy snack using traditional foods, hike through an urban forest making connection with indigenous plants, and participate in a service learning project to remove invasive species and protect biodiversity and water quality.
Science and Medical Track (Oregon Health and Science University)
The science and health track with Oregon Health and Science University (OHSU) exposed youth to different health and science fields at OHSU campus. The workshop provides a connection for youth who are interested in health professions and becoming future healers. Youth expressed interest in the respective fields, pharmacy, dentistry, medicine, ophthalmology, pediatrics, nursing, research, chemist, therapist, nutritionist, psychiatry, and public health!